ASCO Annual Meeting 2026 Colorectal Cancer Updates
The American Society of Clinical Oncology (ASCO) Annual Meeting is taking place May 30 – June 3, 2026 in Chicago, Illinois, bringing together oncologists, researchers, and patient advocates from around the world to share the latest advances in cancer care. This year’s meeting featured several important updates for the colorectal cancer community – here’s what you need to know so far.
Blood test may guide chemotherapy decisions in stage II colon cancer
June 2026 · 2026 ASCO Annual Meeting
A new clinical trial shows that a blood test measuring traces of cancer DNA after surgery can identify which patients are most likely to benefit from chemotherapy – and that treating those patients significantly reduces the risk of recurrence.
What is ctDNA?
After surgery, some patients have tiny amounts of tumour DNA still circulating in their blood – called circulating tumour DNA, or ctDNA. Even when scans appear clear, detectable ctDNA suggests microscopic cancer cells may remain, putting those patients at higher risk of recurrence. Most stage II colon cancer patients do not have detectable ctDNA and do well without chemotherapy. The challenge has been reliably identifying the smaller group who need it.
What did the CIRCULATE trial find?
Patients with detectable ctDNA after surgery were randomly assigned to receive adjuvant (post-surgery) chemotherapy or monitoring alone. The results were striking:

Patients with a negative ctDNA test had excellent outcomes without any chemotherapy, suggesting testing could also help many patients safely avoid unnecessary treatment and its side effects.
What does this mean for patients?
- A ctDNA blood test after surgery may help identify which stage II colon cancer patients are at high risk of recurrence and would benefit from chemotherapy.
- Chemotherapy significantly reduced recurrence in ctDNA-positive patients, cutting the recurrence rate from 62% to 19% in this study.
- Patients with a negative ctDNA test had very good outcomes without chemotherapy, suggesting many may be able to safely avoid treatment side effects.
- This is the first randomized trial to show a treatment benefit from ctDNA-guided decisions in stage II colon cancer specifically.
- The trial was smaller than planned due to early closure, so larger studies are still needed to confirm these results and support guideline changes.
What’s next?
While these results are encouraging, ctDNA testing is not yet standard practice for all stage II colon cancer patients in Canada. Researchers and oncologists will now use this data, alongside other ongoing studies, to consider whether ctDNA-guided treatment should become part of routine care. Private ctDNA testing is currently available in Canada, though its application is limited to prognosis assessment (detecting minimal residual disease) and targeted therapy selection (genomic profiling).
Source: Folprecht G et al. CIRCULATE: a prospective randomized trial of ctDNA-guided adjuvant chemotherapy in mismatch repair–proficient stage II colon cancer. Presented at 2026 ASCO Annual Meeting. J Clin Oncol. 2026;44(17 suppl):LBA3500.
New treatment combination shows strong results for BRAF-mutant metastatic colorectal cancer
June 2026 · 2026 ASCO Annual Meeting
A targeted therapy combination nearly doubled the time patients lived without their cancer progressing compared to standard chemotherapy, in a type of metastatic colorectal cancer (mCRC) defined by a specific gene mutation called BRAF V600E.
What is BRAF V600E and why does it matter?
About 8–10% of patients with mCRC have a mutation in a gene called BRAF V600E. This mutation drives aggressive tumour growth and has historically been associated with poor outcomes on standard chemotherapy. Identifying this mutation through biomarker testing is important because it opens the door to targeted treatments designed specifically for it.
What did the BREAKWATER trial find?
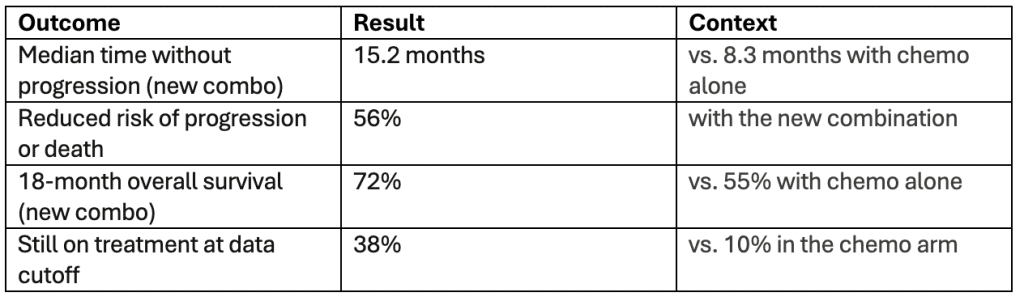
The BREAKWATER trial tested a three-drug combination – encorafenib (a targeted therapy), cetuximab (an antibody therapy), and a chemotherapy regimen called FOLFIRI – as a first-line treatment for patients with BRAF V600E-mutant mCRC. Patients on the new combination went a median of 15.2 months without their disease progressing, compared to 8.3 months on standard chemotherapy.
Overall survival data also favoured the new combination: 72% of patients were alive at 18 months, compared to 55% in the chemotherapy group. The median overall survival had not yet been reached in the new combination arm at the time of analysis.
In February 2026, the US FDA granted traditional approval to encorafenib combined with cetuximab and fluorouracil-based chemotherapy for this patient population, based in part on earlier BREAKWATER data.
“This really allows for improvements in personalized care.”
— Dr. Scott Kopetz, lead study author, MD Anderson Cancer Center, Houston
What does this mean for patients?
- If you have mCRC, ask your oncologist whether your tumour has been tested for the BRAF V600E mutation – knowing your biomarker status can open access to targeted treatments.
- This combination significantly outperformed standard chemotherapy in both delaying progression and improving survival at 18 months.
- The safety profile was manageable and consistent with what is already known about each drug in the regimen.
- In Canada, access to this combination varies. In Ontario, encorafenib received priority access in May 2026 and will be funded under Ontario’s Funding Accelerated for Specific Treatments (FAST) Program for patients with BRAFV600E mCRC. In other provinces, the drug may be funded through a combination of provincial public drug plans, private health insurance, and compassionate access programs. Speak to your care team to learn more.
Source: Kopetz S et al. BREAKWATER: Progression-free and overall survival analyses of first-line encorafenib + cetuximab + FOLFIRI in BRAF V600E-mutant metastatic colorectal cancer. Presented at 2026 ASCO Annual Meeting. J Clin Oncol. 2026;44(suppl 17):LBA3503.