First-line nivolumab plus low-dose ipilimumab for MSI-high/MMR-deficient mCRC
November 2021
Findings from phase II of the CheckMate-142 trial showed that the combination immunotherapy treatment of nivolumab (Opdivo) and low-dose ipilimumab (Yervoy) resulted in meaningful and long-lasting clinical benefit when used to treat patients with microsatellite instability-high (MSI-H)/mismatch repair deficient (dMMR) metastatic colorectal cancer (mCRC) as initial (first-line) therapy. The combination therapy is already approved for use as second-line therapy in this patient population.
Nivolumab is a targeted immunotherapy that blocks the interaction between a specific cell receptor and its partner molecule (ligand) on the surface of important cells of the immune system, known as T cells.
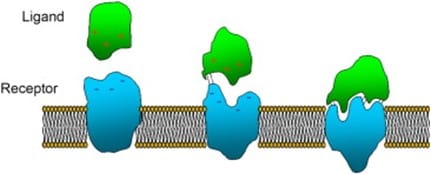
Image source: https://www.sciencedirect.com/science/article/abs/pii/S0928493116307469
When the receptor, known as PD-1, binds to its ligands (PD-L1 and PD-L2), the interaction results in inhibition of the immune system, including anti-cancer activity. In non-cancer states, this interaction is part of our immune system’s natural self-regulating capacity, which prevents it from producing an excessive immune response that could potentially damage the body’s own cells. However, cancer cells can benefit from this immune inhibition by producing greater numbers of the PD-1 ligands. As such, they can stimulate the continued inhibition of active T-cell immune surveillance and remain “invisible” to immune attack. Nivolumab is an antibody that binds specifically to the PD-1 receptor, blocking its interaction with its ligand. This activity lifts the inhibition on the immune system such that anti-tumour immune response can be restored and tumour growth can be reduced.
lpilimumab is an antibody that targets a specific protein (antigen) found on the surface of T cells known as CTLA-4. When the drug binds to CTLA-4, this stimulates T cell activation and proliferation, which contributes to T cell mediated anti-tumour activity.
The study
CheckMate-142 trial enrolled 74 patients who had MSI-H/dMMR mCRC and had not received any previous therapy for metastatic disease. Study participants received nivolumab plus low-dose ipilimumab. Breaks in treatment of less than 6 weeks were allowed to manage any treatment-related toxicities.
38% of participants had tumours with BRAF mutations, and 22% had tumours with KRAS mutations.
Disease control rate was 84% and objective response rate was 69%, with 13% of participants experiencing a complete response rate. Clinical benefit was seen regardless of participants’ BRAF or KRAS mutation status. Grade 3-4 treatment-related adverse events occurred in 22% of patients, and 13% had to stop patients because of any-grade treatment-related adverse events.
Conclusion
The researchers conclude that nivolumab and low-dose ipilimumab showed robust and durable clinical benefit and was well tolerated as an initial therapy for MSI-H/dMMR mCRC. The confirmatory phase III trial, CheckMate-8HW is currently in progress.
Take away message:
For patients with MSI-H/dMMR mCRC, the combination therapy of nivolumab and low-dose ipilimumab showed robust and long-lasting responses as initial, first-line treatment.