ASCO GI 2022: Trial evaluating immunotherapy in neoadjuvant setting for the treatment of locally advanced rectal cancer
January 2022
Total neoadjuvant therapy (TNT) is a standard approach for the treatment of locally advanced rectal cancer (stage II/III) that has been shown to produce better pathologic complete response (pCR), as well as improvements to disease-free survival (DFS), overall survival (OS), while reducing the risk of distant metastasis[1].
Neoadjuvant therapy: therapy such as radiation or chemotherapy that is given before a main treatment, which is usually surgery.
Pathologic complete response: the lack of all signs of cancer in tissue samples removed after treatment with chemotherapy or radiation.
Disease-free survival: the amount of time a patient lives after treatment during which there are no signs and symptoms of the disease.
Overall survival: the time which begins at diagnosis or at the start of treatment up to the time of death.
TNT aims to deliver an intensive pre-surgical, neoadjuvant treatment regimen to patients with rectal cancer through the combination of systemic chemotherapy with chemoradiation to improve pCR and survival rates.
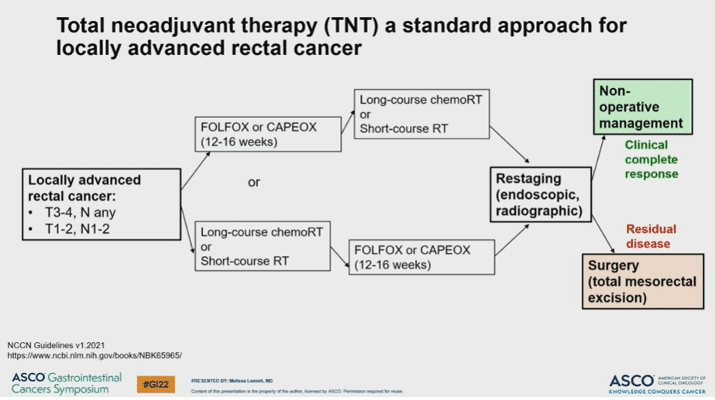
Neoadjuvant chemotherapy in TNT usually consists of the combination regimens of FOLFOX (folinic acid, fluorouracil and oxaliplatin) or CAPOX (capecitabine and oxaliplatin). This is either preceded or followed by chemoradiation consisting of either short-course or long-course radiation (choice between short-course and long-course radiation based on cancer centre protocol and patient’s needs and preferences). This is followed by restaging of the cancer, and the option to proceed to surgery or not depending on the patient’s response to neoadjuvant therapy.
Key considerations about rectal surgery
Rectal surgery is associated with higher rates of complications (e.g. sexual dysfunction, incontinence). As such, patients with rectal cancer who achieve a complete pathological response after neoadjuvant therapy may be considered for non-operative management, also known as “watch and wait” (WW). WW consists of very close surveillance and follow-up of patients who have achieved a complete response after TNT with the goal of avoiding surgery unless it is needed, such as in the case that the cancer comes back (cancer recurrence).
The study
MSI-H/dMMR tumours make up about 5-10% of all rectal cancer, and patients with this type of tumours have been shown to have an increased chance of progressing on neoadjuvant chemotherapy. While advanced rectal cancer that is microsatellite instability high (MSI-H)/mismatch repair deficient (dMMR) may be treated with immunotherapy, the use of immunotherapy in the neoadjuvant setting in patients with locally advanced disease has not been explored.
A recent phase II study (NCT04165772) aimed to evaluate the early use of immunotherapy as part of TNT for patients with locally advanced rectal cancer (stage II/III). Patients with stage II/III MSI-H dMMR rectal cancer received neoadjuvant immunotherapy (dostarlimab) with or without chemoradiation as part of TNT for a total of 6 months. Patients first received immunotherapy, and those with any remaining disease after 6 months of treatment went on to receive standard chemoradiation. Following chemoradiation, any patients that did not reach a complete response were managed surgically.
Findings
Among the 13 patients enrolled in the study, none have required chemoradiation or surgery, and none have experienced any serious adverse events. As such, treating this subset of patients with neoadjuvant immunotherapy appears to be an effective and well-tolerated treatment that allows patients to avoid chemoradiation and surgery entirely, representing a novel strategy for treating MSI-H/dMMR rectal cancer. Long-term follow up and expansion of the study to evaluate this treatment approach in a larger patient population is ongoing.
Take away message:
The use of immunotherapy in the neoadjuvant setting appears to be a safe, effective and well-tolerated treatment for patients with MSI-H/dMMR locally advanced rectal cancer.
[1] https://theoncologist.onlinelibrary.wiley.com/doi/full/10.1002/onco.13824#:~:text=The%20role%20of%20total%20neoadjuvant,survival%20compared%20with%20standard%20treatment.